|
Interesting patient stories have emerged, as we collect clinical data for our MS study. The stories presented here are true, but are abridged or altered somewhat to avoid disclosing personal health information (PHI). PHI is protected by law, which we take seriously. But some patients have given us specific permission to talk about their cases. As for the data, we have tested ten bacterial antigens in the lab, derived from bacteria we grew in culture here at the University of Utah and at the Intermountain Medical Center Microbiology Laboratory. These antigens are our markers for MS detection. (A preprint describing this work in detail is available here.) Please see the list of definitions at the end of the article, for help with medical acronyms. The following five stories open doors into our understanding of MS. MS-10 is a middle-aged woman with progressive MS. She has experienced a multitude of neurologic symptoms starting with hearing difficulties, then difficulty walking, generalized weakness, followed by speech difficulties. She is now confined to a wheelchair. The neurologists have called her syndrome “atypical MS” with severe neurodegeneration. Spinal fluid analysis shows relatively low antibody levels and intact BBB, but a markedly elevated IgG index and several OCBs are present. This indicates that antibodies against something are being made in the brain and spinal fluid. Cracking the MS Code study result: Her spinal fluid has detectable antibodies against all ten MS bacteria, and is strongly reactive against three of the MS bacteria. However, none of these spinal fluid reactivities were higher than expected based on the reactivity of her blood serum. Comment: Although this patient’s spinal fluid has a relatively low amount of total antibodies (IgG), they seem to be directed against our MS antigens, and three in particular: Akkermansia, Atopobium, and Cutibacterium. It will be interesting to see if any of the OCBs in her spinal fluid bind to any of these MS candidate bacteria. That is, are any of her OCBs (which are, by definition, IgG antibodies in spinal fluid) directed against our MS bacteria? If so, we could reasonably conclude that one or more of these bacteria set off her demyelinating disease.
MS-13 is an older pre-diabetic man who developed a tremor and hand weakness. Evaluation showed a lesion in the medulla, deep in the brain. Multiple tests for infection came out negative, but for some reason the patient was treated with eight weeks of intravenous antibiotics and steroids. The medulla lesion improved and so did his symptoms. He is no longer receiving neurology care. The diagnosis was felt to be ADEM, an MS-like disease that typically does not recur. (Multiple sclerosis recurs multiple times, whereas ADEM patients have just one demyelinating episode.) The patient’s spinal fluid IgG index was high (antibodies made within the brain), his albumin index was high (leaky BBB), but the OCB test was negative. Cracking the MS Code study result: Antibodies were detected in his spinal fluid against all six MS bacteria tested, and three of those were strongly reactive. Comparisons to serum reactivity were not possible because no serum was collected at the time of his illness. Question: What antibiotic did this man receive? Did it actually help limit his disease? Answer: We don’t know. Likely, the doctors prescribed an antibiotic that gets into the brain well, like ceftriaxone. We can’t say for sure if the antibiotics or the steroids limited his disease. We can only determine this by a well-designed study involving many such patients. MS-82 is a young woman who developed myelitis (spinal cord inflammation) following a two week flu-like illness with fatigue. She presented to the hospital with neurologic symptoms that included tingling in her legs and difficulty walking. She had a spinal tap just two days later. MRIs showed areas of demyelination in both the brain and spinal cord. Spinal fluid studies showed a leaky BBB, but no elevation in spinal fluid antibodies and no OCBs. She improved somewhat with aggressive immune suppression. She has a relatively severe form of demyelinating disease with MS-like symptoms involving both the brain and spinal cord. Cracking the MS Code study result: This patient has detectable antibodies against nine of the ten MS bacteria, two strongly reactive (Lactobacillus, Cutibacterium). We also see evidence for extra antibodies in the spinal fluid (intrathecal antibody production), compared to those found in her blood, against five of these bacteria. Question: Are the antibodies in her spinal fluid, particularly those made in excess, directed against anything in particular? Answer: Yes, they seem to be directed at some of the MS antigens we tested. We applaud the doctors for stepping in so early to help this patient. It seems likely that she may have now developed an immune response in her spinal fluid (i.e. OCBs), and that the first test was done too soon—after only two days of neurologic symptoms—to detect the bands. It would be ideal to retest her spinal fluid and see if the antibody response or OCBs have developed.
MS-03 is a relatively young Idaho rancher whose case proved to be uniquely interesting. This man and his family have been outspoken about his disease, both in the local media and as the subject of an ESPN feature video. The inciting event was believed to be an attempted winter rescue of a distressed newborn calf, possibly leading to inhalation of aerosolized bacteria in the enclosed pickup truck. This was followed by a brief febrile illness and then progressive neurologic dysfunction over the course of several weeks, with ADEM as the final neurologic diagnosis. Sequencing of a small diagnostic brain biopsy of this patient revealed lactobacillus as the most abundantly mapped microbe at the genus level. Lactobacillus is found in the female genital tract of many mammals, including humans, where it is dominant, and in cattle including newborn calves. Cracking the MS Code study result: This subject’s CSF was highly reactive against five of the tested bacterial antigens, with the highest EI against Lactobacillus paracasei among all the subjects tested. However, the spinal fluid antibodies against lactobacillus were not higher than expected, arguing against a causative role for lactobacillus in his disease. In an attempt to prove causation, OCBs were retested, but they did not survive prolonged freezing. Comment: It is plausible that this subject’s ADEM was triggered by microbes, including Lactobacillus, encountered from an exposure to a newborn calf. However, the data is not completely conclusive. The patient has recovered as much as possible, but still has some difficulties with activities. He continues to coach basketball and live with his family.
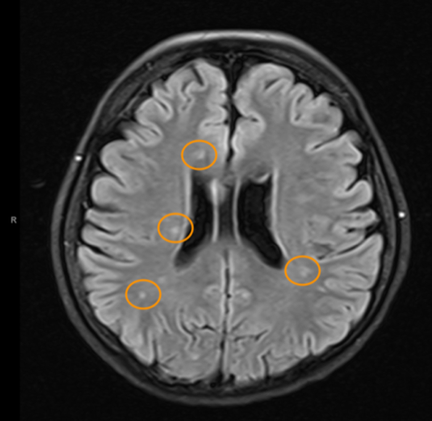
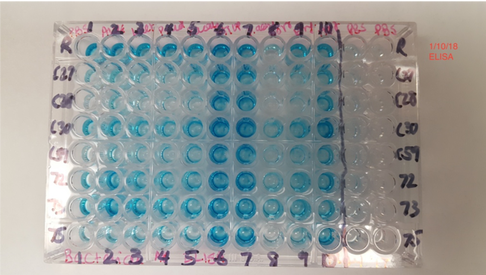
The blue color indicates binding of antibodies in spinal fluid to the antigens on the plate (i.e. CSF reactivity). The preliminary testing shown here was not used for the final analysis. MS-85 is a young woman who presented to the hospital with a new onset of seizures. Her seizures were unprovoked and not associated with fever or medication use. They were generalized (“grand mal”) and witnessed by her family and then the hospital staff. Brain MRI imaging showed a “temporal lobe T2/FLAIR hyperintensity” and “additional predominantly frontal white matter T2/FLAIR hyperintensities.” Spinal fluid testing showed an elevated IgG Index and numerous OCBs. BBB was intact and total IgG in the spinal fluid was normal. Apart from seizures, this woman had no neurologic signs or symptoms.
Cracking the MS Code study result: This patient’s CSF was reactive against all ten tested bacterial antigens, and strongly reactive against Cutibacterium and Akkermansia. Spinal fluid reactivities were higher than expected based on the reactivity of her blood serum against six of the MS candidate bacteria. CSF reactivities were 50-60% higher than expected against Lactobacillus, Pseudomonas, and Bacteroides. Comment: About 10% of MS cases present with seizures. A focal lesion in the temporal lobe is the likely cause of MS-85’s seizures. The areas of frontal lobe demyelination likely went unnoticed, or the symptoms were subtle (e.g. cognitive difficulties) and were well compensated. Testing suggests that the IgG immune response in her CSF is directed against several MS candidate bacteria. This is evidence that bacteria (particularly Lactobacillus, Pseudomonas, and Bacteroides) played a role in her demyelination and seizures. Despite all this, she has done well without specific treatment of her MS. Conclusions It’s clear from the above cases that demyelinating diseases present in a variety of ways, with different symptoms and outcomes. It is also clear that the spinal fluids of patients with demyelinating diseases have antibodies directed against some or most of our MS candidate bacteria. In some cases, the levels of these antibodies are higher than expected. Sometimes we can show that these anti-bacterial antibodies were made in the brain and spinal cord, and did not just leak in from the serum, especially in cases where the BBB is intact. These findings may be illuminating the causes of MS. The facts don’t lie, and it’s up to us to interpret them correctly. Acronyms and definitions Demyelination = the process of myelin destruction in the brain and spinal cord. Myelin is a fatty substance that acts as insulation between nerve fibers. BBB = blood-brain barrier. This normally functions to keep cells, toxins, and big molecules like antibodies in the blood and out of the brain and spinal fluid. IgG = Immunoglobulin G. These are the main forms of antibodies found in human spinal fluid. MRI = magnetic resonance imaging. This is the brain imaging technique generally used to show demyelination and confirm the diagnosis of MS. NMO = neuromyelitis optica. This is an MS-like disease that tends to be severe, usually involving the spinal cord and optic nerves. ADEM = acute disseminated encephalomyelitis. An acute MS-like illness that occurs only once and does not recur. OCB = oligoclonal bands. These are IgG antibodies found in the spinal fluid and not in the blood. They consist of a few (oligo) clones (species) of antibodies visualized on a gel (bands). They are direct evidence of antibody production in the brain or spinal cord. Their intended targets remain unknown. Some researchers believe they are the key to finding the cause of MS. IgG Index = a calculated value that compares IgG antibodies in the spinal fluid and serum to albumin in the spinal fluid and serum. Elevated values of the IgG index are evidence of antibody production in the brain or spinal cord.
0 Comments
|
AuthorDr. John Kriesel is Associate Professor of Infectious Diseases at the University of Utah School of Medicine. He began this blog to raise awareness and generate discussion about the possible causes of multiple sclerosis. Archives
March 2021
Categories |
 RSS Feed
RSS Feed